Preparing your patients for IMCIVREE treatment
Once-daily administration of IMCIVREE can help reduce BMI and hunger1
Subcutaneous injection, administered1:
- At the beginning of the day
- With or without food
- In the abdomen, thigh, or arm, rotating injection sites daily
IMCIVREE can be self-administered or given by a caregiver. Refrigerated storage is recommended, with room temperature storage permitted for up to 30 days.1

Reestablishing MC4R pathway function through continuous treatment with IMCIVREE is foundational for effective long-term treatment of acquired HO.1

Find out how Rhythm InTune provides injection training for patients and caregivers.
Learn MoreFollow the titration schedule to reach a maintenance dose to optimize efficacy and tolerability1
| Young Children (4 to <6 years of age)1 | ||||
|---|---|---|---|---|
| Baseline body weight | Weeks 1-2 (Starting Dose) | Weeks 3-4 | Weeks 5-6 | Week 7 and onward |
| 15 to <20 kg (33 to <44 lbs) | 0.5 mg once daily (recommended maintenance dose) | |||
| 20 to <30 kg (44 to <66 lbs) | 0.5 mg once daily | 1.0 mg once daily (recommended maintenance dose) | ||
| 30 to <40 kg (66 to <88 lbs) | 0.5 mg once daily | 1.0 mg once daily | 1.5 mg once daily (recommended maintenance dose) | |
| ≥40 kg (≥88 lbs) | 0.5 mg once daily | 1.0 mg once daily | 1.5 mg once daily | 2.0 mg once daily (recommended maintenance dose) |
If the starting
| ||||
When the child reaches age 6, the maintenance dose increases to 3.0 mg regardless of weight.1
| Adults and children (≥6 years of age)1 | |||
|---|---|---|---|
| Weeks 1-2 (Starting Dose) | Weeks 3-4 | Weeks 5-6 | Weeks 7 and onward |
| 0.5 mg once daily | 1.0 mg once daily | 2.0 mg once daily | 3.0 mg once daily (recommended maintenance dose) |
If the starting
| |||
No dose adjustments are needed for patients with mild to moderate renal impairment. IMCIVREE is not recommended for use in patients with acquired HO and severe renal impairment or in patients with end-stage renal disease.1
Select Monitoring Information
For patients with secondary adrenal insufficiency1:
Patients with acquired HO and secondary adrenal insufficiency reported serious adverse reactions related to acute adrenal insufficiency in 5% of IMCIVREE-treated patients and no placebo-treated patients. In patients with secondary adrenal insufficiency, monitor for clinical signs of acute adrenal insufficiency.
For patients with central diabetes insipidus1:
Patients with acquired HO and concomitant central diabetes insipidus (DI)/arginine vasopressin (AVP) deficiency reported hyponatremia in 6% of IMCIVREE-treated patients and 2% of placebo-treated patients and hypernatremia in 5% of IMCIVREE-treated patients and 4% of placebo-treated patients. Monitor serum sodium levels with changes in fluid intake and hydration status. Adjust the doses of concomitant therapies for DI/AVP deficiency as needed.
Patients with pre-existing DI/AVP deficiency and/or secondary adrenal insufficiency should be monitored and counseled as outlined in the PI. Endocrinologists should review patients’ existing coordination plans once they start IMCIVREE to help manage these conditions and adjust concomitant therapies as needed.
Effective, long-term weight management starts with setting patient expectations
In clinical trials, it took some time for weight and hunger reductions to be noted, while patients experienced certain AEs soon after starting treatment. This chart highlights some of the most common AEs, but it does not include all reported AEs.1,2
Timing of common effects seen in clinical trials1,2
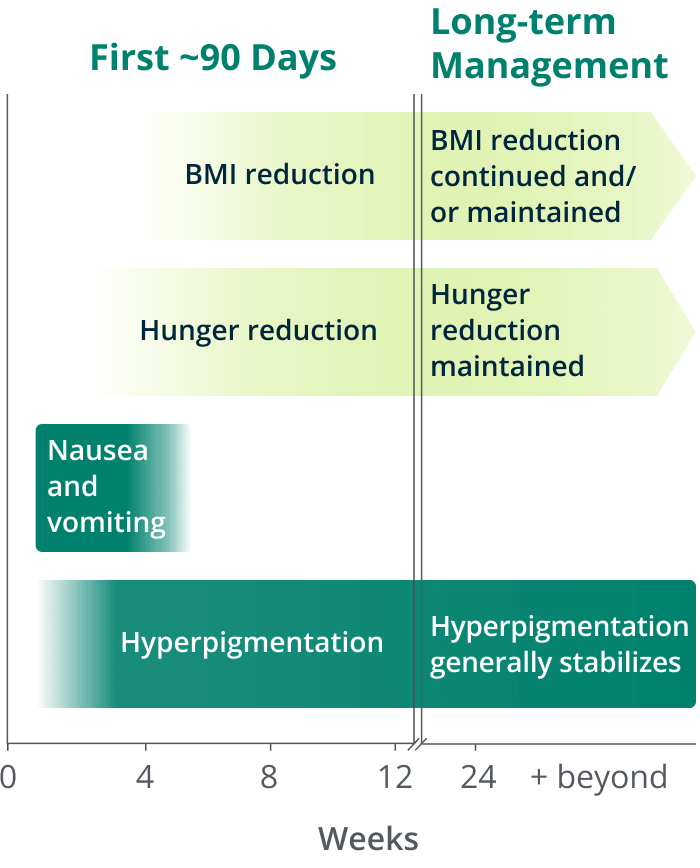
BMI reduction
Improvement was evident within 4 weeks of initiation and continued with ongoing treatment.1
Hunger reduction
Improvement was reported soon after treatment initiation and was maintained with ongoing treatment.1
Nausea and vomiting
Events occurred most frequently within the first month of treatment, then declined.1
Hyperpigmentation
Hyperpigmentation increased throughout the dose escalation period and generally plateaued in the initial months of treatment.1,2
Achieving the benefits of treatment with IMCIVREE may take time. Talking to patients about when they can expect weight and hunger benefits and common adverse reactions may help them manage through the short-term treatment initiation to achieve their longer-term goals.
Find resources for your practice and for your patients considering IMCIVREE.
Start prescribing IMCIVREE and learn about patient support.
AEs=adverse events, BMI=body mass index, HO=hypothalamic obesity, kg=kilogram, lbs=pounds, MC4R=melanocortin-4 receptor, mg=milligram.