Significant improvements in weight and hunger for children1
In patients 4 years and older
IMCIVREE delivered rapid, significant, and sustained weight loss1,2
142 patients participated in the Phase 3, double-blind, multicenter, placebo-controlled pivotal trial of IMCIVREE in acquired HO (IMCIVREE, n=94; placebo, n=48)1
Primary Endpoint: BMI Mean Percent Change From Baseline by Treatment Group (N=142)1*
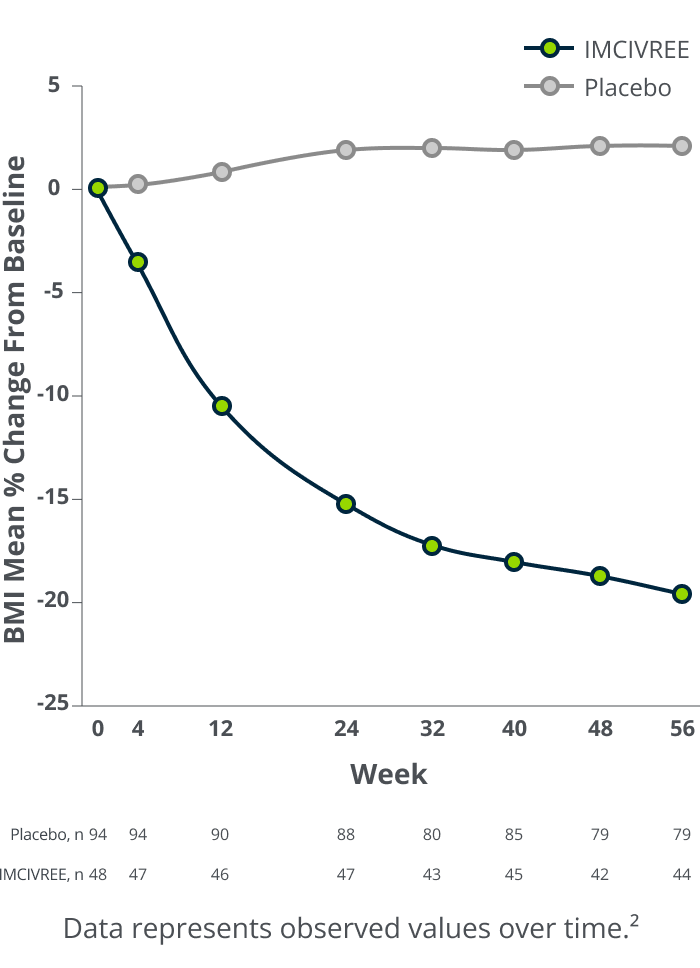
18.4% placebo-adjusted reduction in BMI
at 52 weeks on a therapeutic dose*
15.8% mean reduction for IMCIVREE vs 2.6% mean increase for placebo (p<0.0001)1
- 18.2% placebo-adjusted reduction in BMI for patients 4 to <18 years old (n=76; 15.3% mean reduction for IMCIVREE vs 3.0% mean increase for placebo)2
- 18.8% placebo-adjusted reduction in BMI for patients 18 years and older (n=66; 16.6% mean reduction for IMCIVREE vs 2.2% mean increase for placebo)2
*IMCIVREE=94; placebo=48. LSM difference (95% CI: −21.9, −14.9).
15.2-cm placebo-adjusted reduction in waist circumference, indicative of reduced adiposity2,3
- Mean reduction of 12.0 cm in waist circumference for IMCIVREE vs mean increase of 3.2 cm for placebo at 52 weeks (N=142)†
- Waist circumference is a validated surrogate marker for excess adiposity
- This endpoint was not included in the statistical testing hierarchy and was not controlled for multiplicity
†IMCIVREE=94; placebo=48.
In patients 4 to <18 years old
IMCIVREE improved weight trajectory and helped pediatric patients achieve a healthier weight class2
Representative Weight Trajectory for a Pediatric Patient With Acquired HO Before and After IMCIVREE2

26-point mean reduction
in the BMI percent of the 95th percentile for IMCIVREE
vs 0.6-point mean reduction for placebo2
43% (20/46) of pediatric patients achieved a BMI <95th percentile with IMCIVREE, below the threshold for obesity.2
This chart applies mean trial data to a representative BMI trajectory in acquired HO to show what a pediatric patient taking IMCIVREE may experience after 1 year. BMI at the start of IMCIVREE treatment and after 1 year with IMCIVREE reflect mean values for pediatric patients in the Phase 3 trial. This growth chart is for illustrative purposes only.2
Changes in Weight Classification for Patients 4 to <18 Years Old With IMCIVREE2‡
9% (4/46) reduced by 3
weight classes
35% (16/46) reduced by 2
weight classes
26% (12/46) reduced by 1
weight class
Weight Classes Based on BMI Percentile:
Obesity class III: ≥140% of the 95th percentile
Obesity class II: ≥120% to <140% of the 95th percentile
Obesity class I: ≥95th percentile to <120% of the 95th percentile
Overweight: ≥85th percentile to <95th percentile
Healthy weight: ≥5th percentile to <85th percentile
‡Baseline and observed Primary Timepoint values utilized for comparison. Three IMCIVREE patients did not have an observed Primary Timepoint Value indicated and are not included in the analysis. Thirteen patients were in the same weight class between Baseline and the Primary Timepoint. One patient increased a weight class.2
In patients 12 years and older
IMCIVREE delivered significant hunger reduction1
Key Secondary Endpoint: Hunger Mean Change From Baseline by Treatment Group in Patients ≥12 Years (n=110)1§

2.3-point mean reduction
in daily most hunger score for IMCIVREE
vs 1.4-point mean reduction for placebo (p=0.04).1||
§IMCIVREE=74; placebo=36. Patients 12 years and older who were able to self-report their hunger recorded their maximal hunger ("most hunger") each day on an 11-point scale from 0 ("not hungry at all") to 10 ("hungriest possible").
||LSM difference: −0.8 (95% CI: −1.62, −0.02).
Impact on symptoms of hyperphagia
Patients 12 years and older who were able to self-report were also administered the Symptoms of Hyperphagia questionnaire. Based on their responses, the Symptoms of Hyperphagia Composite Score decreased from baseline to 52 weeks.2
Formal validation has not been completed for the instrument used to measure symptoms of hyperphagia in the acquired HO population. This endpoint was not powered for formal testing or significance.
Additional efficacy measures for pediatric patients
Because she's not constantly stressing over food and when her next meal will be and what she can eat and how much she can eat, she's not in distress constantly.
– Caregiver of a patient on IMCIVREE
She is glad that she’s losing weight and is enjoying these moments with friends and family.
– Caregiver of a patient on IMCIVREE
Individual results may vary.
Get your patient started with IMCIVREE.
See efficacy data for IMCIVREE in adults.
BL=baseline, BMI=body mass index, CI=confidence interval, cm=centimeter, HO=hypothalamic obesity, kg=kilogram, m=meter.